Today, CPR is more standardized, data-driven, and accessible than at any point in history. What was once based on trial-and-error has evolved into a highly refined, evidence-based intervention guided by organizations like the American Heart Association (AHA), International Liaison Committee on Resuscitation (ILCOR), the Health & Safety Institute (HSI), and the American Red Cross. These groups continuously analyze global research and update protocols to reflect what actually improves survival outcomes.
At the center of modern resuscitation is the concept of high-quality CPR. This is not just about “pushing on the chest”—it is about doing it correctly, consistently, and with precision. Current guidelines emphasize:
- Compression depth: at least 2 inches (5 cm) in adults
- Compression rate: 100–120 compressions per minute
- Full chest recoil: allowing the heart to refill between compressions
- Minimizing interruptions: keeping pauses under 10 seconds
These details matter. High-quality compressions directly impact coronary and cerebral perfusion—the blood flow to the heart and brain—which are the two organs most critical to survival.
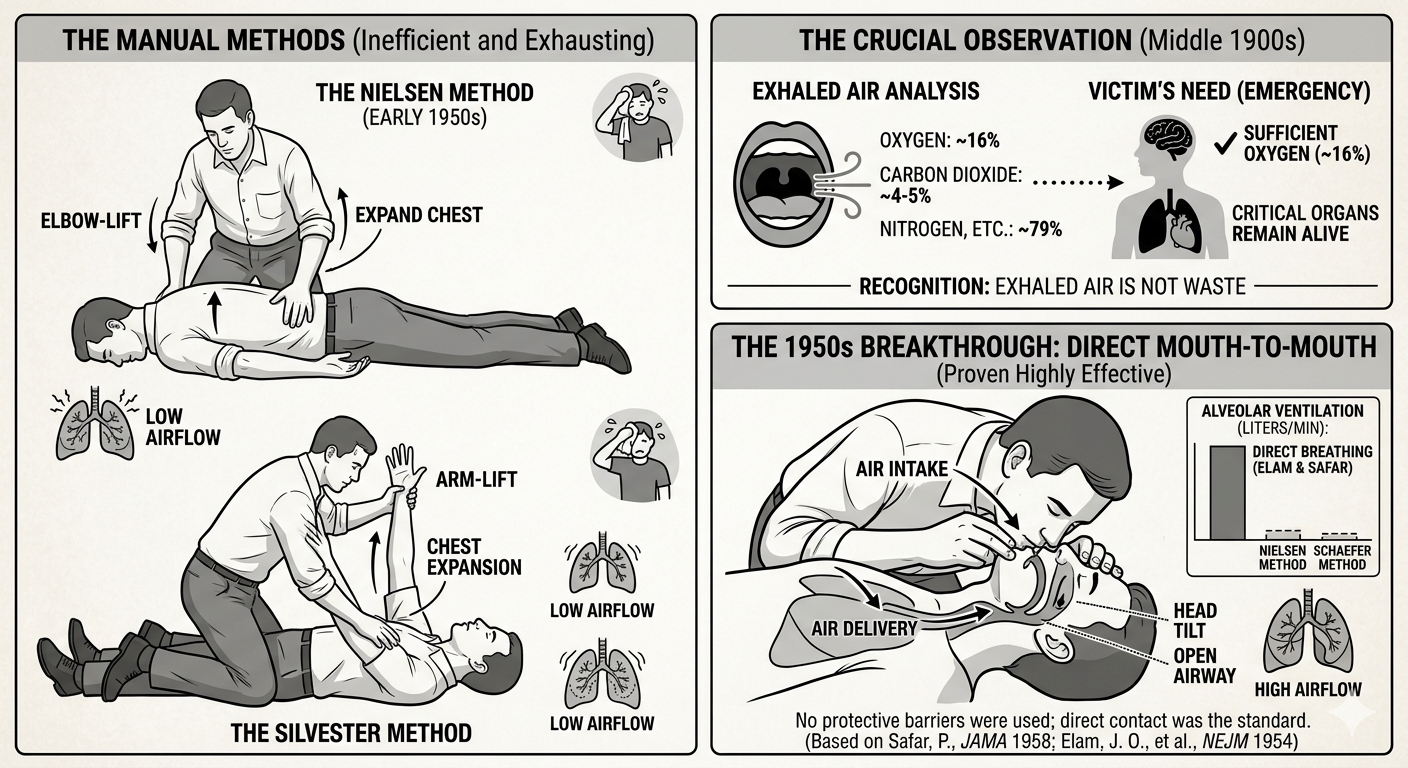
Another major shift in the modern era is the widespread adoption of Hands-Only CPR. Research published in Circulation demonstrated that for adult sudden cardiac arrest, compression-only CPR can be just as effective as traditional CPR in the first few minutes. This simplified approach removes one of the biggest barriers for bystanders: hesitation around mouth-to-mouth contact.
Hands-Only CPR is straightforward:
- Call 911
- Push hard and fast in the center of the chest
By eliminating complexity, more people are willing to act—and early action is what saves lives. This approach has been heavily promoted in public awareness campaigns because it increases bystander intervention rates, which historically have been a weak link in the “chain of survival.”
Technology has further transformed how CPR is delivered. Today, rescuers may be supported by:
- AEDs with real-time feedback, correcting compression depth and rate as you work.
- Smartphone apps that alert nearby trained responders to cardiac arrests in public places.
- Dispatcher-assisted CPR, where 911 operators coach callers step-by-step through the process.
- Wearable devices and AI systems that can detect cardiac events earlier than ever before.
Despite these advancements, one constant remains: the first few minutes still belong to the bystander. EMS response times, even in optimized systems, cannot compete with immediate action from someone already on scene. That is why modern CPR training focuses not only on technique, but also on confidence, speed, and decision-making under pressure.
In many ways, CPR has come full circle. While the tools and science have advanced dramatically, the core principle is unchanged: ordinary people stepping in to help another person in their most critical moment. From 18th-century resuscitation attempts using bellows, to today’s data-driven protocols and smart defibrillators, the mission has remained consistent—preserve life, protect the brain, and restore the heartbeat.
Learning CPR today means stepping into that legacy with the best tools and knowledge available.
Your training should reflect the modern standard.
Stay current with the latest guidelines from the American Heart Association and the American Red Cross. Get hands-on, practice with real equipment, and build the confidence to act when it matters most. Secure your spot in an upcoming class at ResqTraining.com.
Sources for Part 6:
- Sayre, M. R., et al. (2008). Hands-Only (compression-only) cardiopulmonary resuscitation. Circulation.
- International Liaison Committee on Resuscitation (ILCOR). 2020 International Consensus on CPR.
- American Heart Association. High-Quality CPR Data & Guidelines (2020).
- American Red Cross. Modern CPR Training and Accessibility Guidelines.