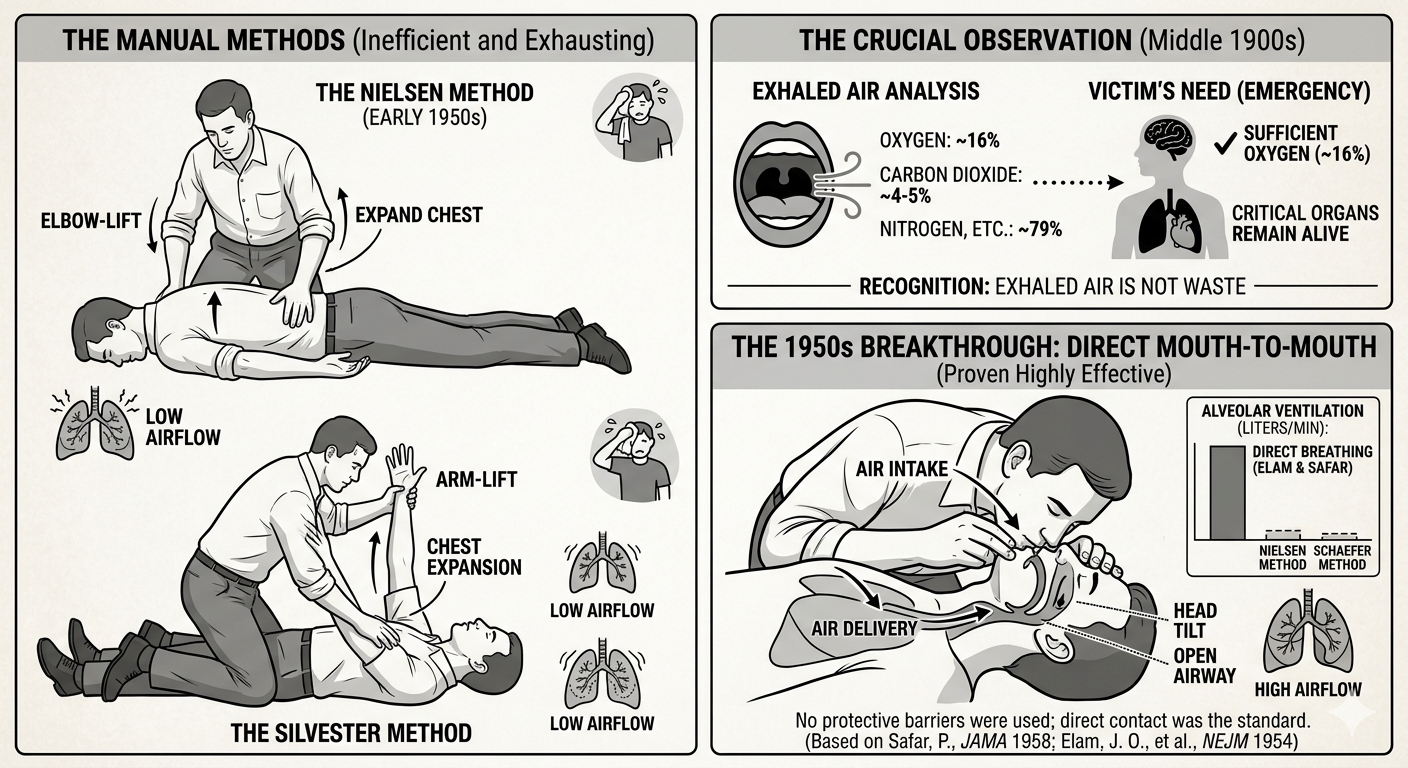
In the middle of the 1900s, scientists made a big discovery. They found that human breath still has enough oxygen to help someone else. Before this, many people believed that the air we breathed out was just waste. However, researchers discovered that while we breathe in about 21% oxygen, we only use a small amount of it. This means the air we breathe out still contains around 16% oxygen. This is more than enough to keep another person’s brain and organs alive during an emergency.
Before mouth-to-mouth became the standard, rescuers used several manual techniques that relied on body movement:
- The Silvester Method: This involved laying the victim on their back and raising their arms above their head to expand the chest, then pressing the arms against the chest to force air out.
- The Schaefer Method: To avoid the tongue blocking the airway, the victim was placed face-down. The rescuer would kneel over them and press on the lower back to push air out, then release to let air in.
- The Holger Nielsen Method: Popular in the early 1950s, this combined the two. The victim was face-down, and the rescuer would pull the victim’s elbows upward to expand the chest, then press on the back to exhale.
While these were popular, they were very exhausting and moved very little air compared to direct breathing.
During the 1950s, Dr. James Elam and Dr. Peter Safar proved that direct mouth-to-mouth breathing was much more effective. They conducted experiments showing that a rescuer could maintain healthy oxygen levels in a victim just by using their own breath. Interestingly, they initially experimented with “mouth-to-nose” breathing as well, believing it might be easier to create a seal. However, they eventually settled on mouth-to-mouth as the primary method because it allowed for a larger volume of air to enter the lungs.
One major difference between then and now was the lack of protection for the rescuer. In the 1950s, there were no breathing barriers or pocket masks. Rescuers were taught to place their mouths directly onto the victim’s face. At that time, doctors were so focused on the survival of the patient that the risk of spreading germs to the rescuer was rarely discussed. It wasn’t until decades later, with a better understanding of infectious diseases, that the medical community developed the one-way valves and barriers we use today.
While these tests often focused on victims of drowning or drug overdoses, doctors realized this method could help in any situation where someone stopped breathing. Because of their hard work, this became a standard way to help victims of drowning, suffocation, and even carbon monoxide poisoning.
Consequently, doctors started to teach this method to others. It was a simple way to help, but the heart still needed more attention. Medical professionals began to notice that even if they could get air into the lungs, the victim’s skin would remain blue and their pulse would remain absent. They realized that oxygen in the lungs was useless if there was no way to transport it to the brain and other vital organs. This critical gap in knowledge meant that while rescue breathing was a massive leap forward, the “engine” of the body—the heart—was still being ignored.
Are you confident in your rescue breathing?
Learn the safest and most effective mouth-to-mouth techniques with professional guidance. Register for training at ResqTraining.com.
Sources for Part 2:
- Safar, P. (1958). Ventilatory efficacy of mouth-to-mouth artificial respiration. JAMA.
- Elam, J. O., et al. (1954). Oxygen and carbon dioxide exchange and alveolar ventilation in mouth-to-mask resuscitation. New England Journal of Medicine.
- National Center for Biotechnology Information (NCBI). The history of the Holger Nielsen method.