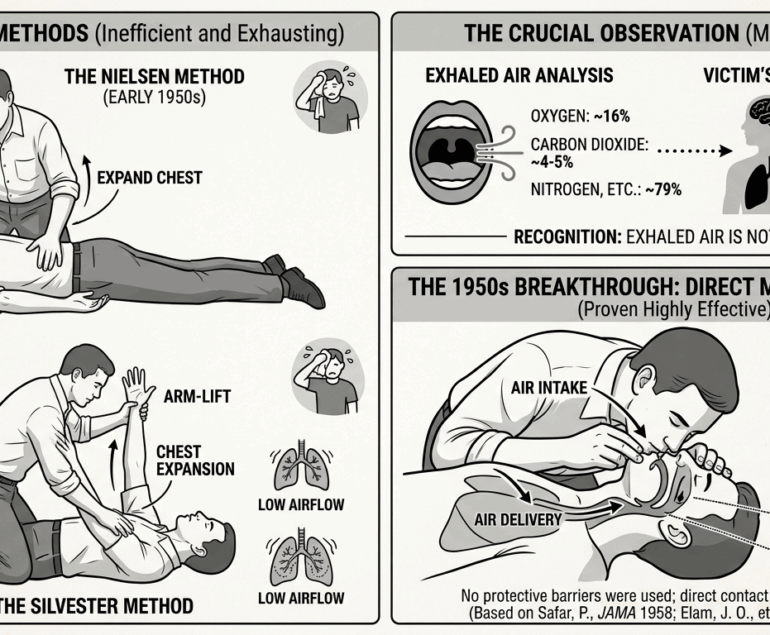
Rescue breathing was a major breakthrough—but it only solved half the problem of cardiac arrest survival. Oxygen could enter the lungs, but without blood circulation, it never reached the brain or vital organs. Within minutes of a heart stopping, the lack of blood flow leads to irreversible brain damage. The missing link wasn’t just air—it was movement.
That changed in 1960 at Johns Hopkins University, when researchers William B. Kouwenhoven, James R. Jude, and Guy Knickerbocker made a discovery that would redefine emergency medicine and the history of cardiopulmonary resuscitation (CPR).
The Breakthrough: Pumping the Heart Without Surgery
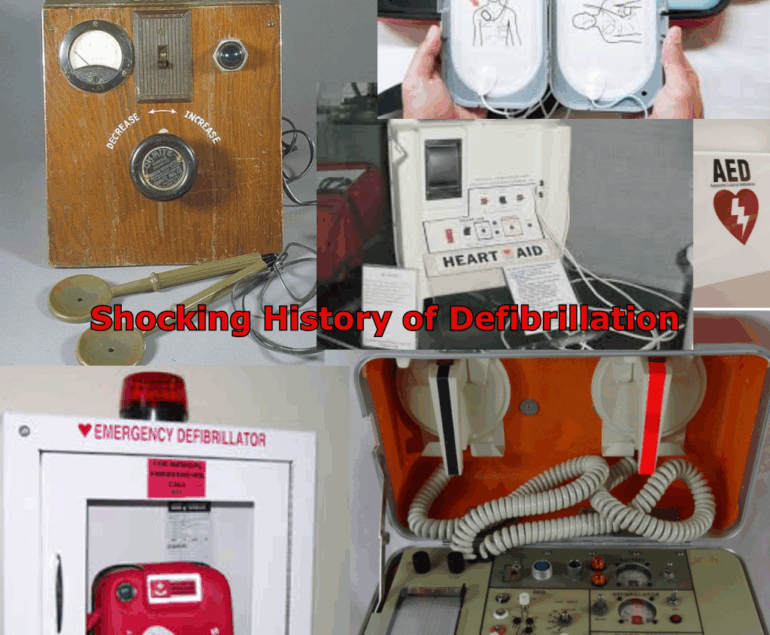
While studying external electrical defibrillation—searching for a way to treat chaotic heart rhythms without invasive surgery—the team noticed something unexpected: Firm pressure applied to the chest could generate a measurable pulse. They realized that the heart could be compressed between two rigid structures:
- The sternum (breastbone) in the front
- The spine in the back
By pressing rhythmically on the sternum, blood was forced out of the heart to the brain and body. Releasing pressure allowed the heart to refill. This technique, known as “closed-chest cardiac massage,” allowed rescuers to circulate blood without opening the chest cavity. This was a massive leap from earlier invasive medical methods such as:
- Open-Chest Cardiac Massage: A surgical procedure requiring a doctor to cut open the chest to manually squeeze the heart.
- Internal Defibrillation: Applying shocks directly to the heart muscle during an operation.
Why Circulation Changed Cardiac Arrest Outcomes
Before this discovery, resuscitation focused almost entirely on ventilation (breathing), and survival rates remained extremely low. Afterward, rescuers could artificially create a heartbeat. This wasn’t just an improvement—it was the foundation of modern life support. Oxygen from rescue breaths could finally reach the brain, preventing cell death.
The Integration of Modern CPR Standards
When chest compressions were combined with rescue breathing, the integration formed what we now know as Cardiopulmonary Resuscitation (CPR). This coordinated system addresses both the lungs (Ventilation) and the heart (Circulation). Organizations like the American Heart Association (AHA) quickly recognized its impact and began standardizing CPR training, laying the foundation for modern emergency response protocols used worldwide today.
The Clinical Reality of High-Quality CPR
Effective chest compressions are the core of cardiac arrest intervention, but they must meet specific clinical standards to be effective:
- Compression Depth: At least 2 inches in adults to adequately squeeze the heart.
- Compression Rate: 100–120 beats per minute to maintain blood pressure.
- Minimal Interruptions: To ensure constant blood flow to the brain.
In a medical emergency, circulation is the top priority, as brain damage begins in as little as 4–6 minutes. This discovery shifted the focus of first aid from a passive concept to an active, life-saving mechanical intervention.
Master the “Missing Piece” of Survival
High-quality chest compressions are the most critical factor in surviving a cardiac arrest. Build your confidence and learn proper hand placement with expert, hands-on CPR certification at ResqTraining.com.
Sources for Part 3:
- Kouwenhoven, W. B., Jude, J. R., & Knickerbocker, G. G. (1960). Closed-chest cardiac massage. JAMA.
- Johns Hopkins Medicine. The History of CPR: The Hopkins Connection.
- American Heart Association. 1960: The birth of modern CPR.